Wednesday, December 21, 2011
Saturday, December 10, 2011
Monday, November 7, 2011

Friday, November 4, 2011
HyperTAG
- The serum triglyceride concentration can be stratified in terms of population percentiles and/or coronary risk (see 'Definitions, epidemiology, and detection' above):
- Normal <150 mg/dL (1.7 mmol/L)
- Borderline high — 150 to 199 mg/dL (1.7 to 2.2 mmol/L)
- High — 200 to 499 mg/dL (2.3 to 5.6 mmol/L)
- Very high — ≥500 mg/dL (≥5.7 mmol/L)
- Although the contribution of triglycerides to cardiovascular risk has been debated in the past, it now seems clear that elevated triglyceride levels are independently associated with cardiovascular risk, particularly coronary risk. It remains uncertain, however, whether this association is causal, such that hypertriglyceridemia, independent of associated lipoprotein, inflammatory and hemostatic abnormalities, causes atherosclerosis. It is also uncertain whether lowering triglyceride levels reduces risk. (See 'Triglycerides and atherosclerosis' above.)
- There are only limited data regarding which patients with hypertriglyceridemia require treatment and on the choice of therapies. (See 'Management' above.)
- Nonpharmacologic interventions such as weight loss in obese patients, aerobic exercise, avoidance of concentrated sugars and medications that raise serum triglyceride levels, and strict glycemic control in diabetics should be first-line therapy in patients with mild-to-moderate hypertriglyceridemia. Other risk factors for cardiovascular disease, such as hypertension and smoking, should also be addressed. (See 'Nonpharmacologic therapy' above.)
In patients with severe hypertriglyceridemia (fasting triglyceride levels above 1000 mg/dL [11.3 mmol/L]), we suggest a very low fat diet (Grade 2C). (See 'Nonpharmacologic therapy' above.) - Options for pharmacologic therapy directed at reducing triglycerides include fibrates, nicotinic acid, and fish oil. (See 'Pharmacologic therapy (including fish oil)' above.)
- For patients with mild to moderate hypertriglyceridemia (150 to 500 mg/dL [1.7 to 5.7 mmol/L]), and even in patients with triglyceride levels as high as 1000 mg/dL (11.3 mmol/L), the main indication for therapy is reduction of cardiovascular (CV) risk. In patients where the goal of therapy is CV risk reduction:
- Decisions about initiating pharmacologic therapy should be based on global cardiovascular risk. Nearly all patients with known coronary heart disease (CHD) or a CHD risk equivalent (table 4) will require therapy. (See "Treatment of lipids (including hypercholesterolemia) in primary prevention", section on 'Deciding whom to treat' and "Treatment of lipids (including hypercholesterolemia) in secondary prevention", section on 'Identification of patients at risk'.)
- For patients with a triglyceride level below 500 mg/dL (5.7 mmol/L) in whom pharmacologic therapy is indicated, we suggest treatment with a statin rather than an agent targeted at reduction of triglycerides (Grade 2B). Given the lack of high quality evidence directly comparing statin therapy with other treatment options, a reasonable alternative in such patients would be to treat them with fibrates, nicotinic acid, or fish oil. (See 'Mild to moderate hypertriglyceridemia' above.)
- In patients with CHD or a CHD risk equivalent (table 4) who have moderate hypertriglyceridemia (200 to 500 mg/dL [2.3 to 5.7 mmol/L]) and are intolerant of statin therapy, we suggest treatment with nicotinic acid or a fibrate (Grade 2C). Treatment with fish oil is a reasonable alternative. (See 'Mild to moderate hypertriglyceridemia' above.)
- For patients with a triglyceride level above 500 mg/dL (5.7 mmol/L) in whom pharmacologic therapy is indicated, we suggest treatment with a fibrate (such as fenofibrate), followed by the addition of a statin once the triglyceride levels are brought down (Grade 2C). Fish oil therapy is also an option. A reasonable alternative would be to treat lower-risk patients with a statin alone and to only add triglyceride-directed therapy in patients with CHD or a CHD risk equivalent (table 4). (See 'Severe hypertriglyceridemia' above.)
- In patients without a prior episode of pancreatitis, we suggest initiating pharmacologic therapy to reduce triglycerides with a goal of preventing pancreatitis when the level exceeds 1000 mg/dL (11.3 mmol/L) (Grade 2C). Even at this level of triglyceride elevation, the risk of pancreatitis appears to be quite small. Patients being treated for prevention of pancreatitis will often require combinations of triglyceride-lowering medications (ie, a fibrate, fish oil, nicotinic acid) to reduce the triglyceride level below 1000 mg/dL (11.3 mmol/L). (See 'Severe hypertriglyceridemia' above.)
- The management of patients with hypertriglyceridemia and acute pancreatitis and/or a prior episode of pancreatitis is discussed separately. (See "Hypertriglyceridemia-induced acute pancreatitis".)
Use of UpToDate is subject to the Subscription and License Agreement.
HyperTAg causing Pancreatitis
Proposed approach to hypertriglyceridemic pancreatitis

Apheresis — Apheresis should be considered to remove triglycerides from serum if the patient does not have concurrent hyperglycemia and there are no contraindications, such as unstable vital signs or inability to tolerate central venous access.
Many case reports and series have described apheresis for HTGP [28-40]. One series of seven patients with an average level of 1406 mg/dL reported a 41 percent decrease in triglyceride levels after one plasma exchange session [35]. In another case report, triglycerides were lowered from 2410 to 138 mg/dL after three days of apheresis [40]. Neither report described the use of adjunctive therapy such as intravenous insulin, intravenous heparin, or oral statins.The most common anticoagulant used during apheresis is heparin, but there are no data to recommend the appropriate apheresis replacement fluid (albumin versus fresh frozen plasma). When plasma exchange is compared with double membrane filtration apheresis, rates of removal of serum lipids have been lower with double membrane filtration apheresis [41].
The main concerns surrounding apheresis include cost and availability. After one cycle, serum triglyceride levels are re-checked and, if less than 500 mg/dL, apheresis is stopped. If the triglyceride rises (above 500 mg/dL), we generally re-treat with apheresis.
Early initiation of apheresis is likely to be beneficial. We generally proceed with apheresis as soon as possible. In a review of 10 patients with HTGP, nine patients received apheresis with IV heparin and insulin within 48 hours of the diagnosis of HTGP with successful outcomes [42].
Insulin — If apheresis is unavailable, if the patient cannot tolerate apheresis, or if the patient's serum glucose level is >500 mg/dL, we use intravenous insulin. Insulin decreases serum triglyceride levels by enhancing lipoprotein lipase activity, an enzyme that accelerates chylomicron metabolism to glycerol and fatty free acids [43,44]. Because HTGP often presents in patients with uncontrolled diabetes, insulin can decrease both triglyceride and glucose levels.
Intravenous insulin may be more effective than subcutaneous insulin in severe cases of HTGP [25,26]. Many regimens have been reported to lower triglyceride levels to less than 500 mg/dL over 3.5 to 4 days [25-27]. We typically initiate an intravenous infusion of regular insulin in 5 percent dextrose at a rate of 0.1 to 0.3 units/kg/hour to maintain blood sugar levels between 150 and 200 mg/dL.Fingerstick glucose levels every four hours are suggested to ensure glucose control, and triglyceride levels should be monitored every 12 to 24 hours with adjustment of the insulin dosage as needed. Intravenous insulin should be stopped when triglyceride levels are <500 mg/dL, which typically occurs within several days.
Insulin and heparin — The role of heparin is controversial. Heparin stimulates the release of endothelial lipoprotein lipase into the circulation [45] and has been used without insulin to manage HTG [42,46,47]. Multiple case reports and series have described the use of heparin and insulin to lower HTG [21-24,48].
Studies have used varying doses of insulin and heparin administered by various routes [21,22,48]. As an example, in two reports subcutaneous heparin at 5000 units twice daily was used with intravenous insulin [22,48]. In both healthy volunteers and dialysis patients, low molecular weight heparin has been found to deplete lipoprotein lipase stores as efficiently as heparin and to retard the metabolism of triglyceride [49,50].Despite the reported success of intravenous heparin in combination with insulin in HTG management, the use of heparin to treat HTGP has come under greater scrutiny. Heparin causes an initial rise in circulating lipoprotein lipase levels that is quickly followed by increased hepatic degradation of heparin [51]. This degradation contributes to further depletion of plasma stores of lipoprotein lipase and results in an increase of levels of chylomicrons [52]. The transient nature of the benefit seen with heparin raises question as to its use as monotherapy or in combination with insulin.
Antihyperlipidemic therapy — Antihyperlipidemic agents (eg, oral gemfibrozil 600 mg twice daily) should be initiated as adjuvant therapy in patients with HTGP. (See "Lipid lowering with fibric acid derivatives" and "Lipid lowering with diet or dietary supplements" and "Treatment of lipids (including hypercholesterolemia) in secondary prevention".)
Long-term therapy — Oral antihyperlipidemic agents and dietary fat restriction may be needed long-term to prevent recurrences of AP and prevent other complications of HTG. Periodic apheresis has been used with some success as continuing therapy after patients have recovered from their initial episode of AP, and particularly in patients who are noncompliant with diet and oral drug therapy [53]. (See "Lipid lowering with fibric acid derivatives" and "Lipid lowering with diet or dietary supplements" and "Treatment of lipids (including hypercholesterolemia) in secondary prevention".)
Pregnancy — The treatment of HTGP does not differ in pregnancy. Several case reports of gestational HTGP have described the use of apheresis [54,55], intravenous insulin and glucose with enteral restriction of triglyceride [56], intravenous heparin [42,46], low fat diet [57], and gemfibrozil. All resulted in the successful control of HTG and delivery of a healthy neonate
Thursday, November 3, 2011
Statin comparision
There are very good reasons to use rosuvastatin over atorvastatin. Crestor is not a CYP3A4 substrate (Lipitor is), Crestor has only minor actitive metabolites (Lipitor has several very active metabolites), and Crestor is hydrophilic whereas Lipitor is not; hydrophilicity appears to minimize entry into muscles and minimizes muscle pain complaints.
Lipitor differs from simvastatin only in efficacy. If you don't like simva you shouldn't like Lipitor. Pravastatin, although the least potent, is not a 3A4 suThere are very good reasons to use rosuvastatin over atorvastatin. Crestor is not a CYP3A4 substrate (Lipitor is), Crestor has only minor acbstrate and is hydrophilic. It is a good first choice for many.
with all the publicity over rhabdomyolysis at the 80 mg dose, the fact that simvastatin is markedly inferior to atorvastatin (both in hard endpoint trials like IDEAL and in 'softer' surrogate marker studies), and that simvastatin is by far and away the most prone to drug interactions through CYP3A4 of all the statins (witness the labelling revisions for amiodarone, verapamil, diltiazem on top of the previous litany of azole antifungals, antivirals, etc). Quite simply, this statin sucks! It is also the most myopathic of all the statins and the dose-response curve and renal clearance are worrisome. More than 40% of patients in SHARP discontinued it.
Sunday, October 16, 2011
Extubation criteria :
Most parameters of respiratory mechanics are useful only for predicting successful SBT and perform moderately or poorly with extubation prediction. We therefore present a brief discussion of these parameters.
Rapid shallow breathing index (RSBI - f/V T )
Capdevila [16] found significantly lower values of f/V T (50 ± 23 vs. 69 ± 25 breaths/min/l) in successfully extubated patients. Recently a cut off value of RSBI ≥ 57 was described [22] to separate patients who could not be extubated successfully. Epstein, [27] however, found that with f/V T < 100, 14 (of 84) patients failed extubation, 13 due to other organ system problems and suggested that f/V T was not physiologically suited to predict extubation failure. Other studies [2],[20],[29] have also reported inability of f/V T for predicting extubation outcome.
Airway occlusion pressure at 1 s (P 0.1 ) and Ratio of occlusion pressure to maximum inspiratory pressure (MIP) [P 0.1 /MIP]
P 0.1 /MIP is an index of balance between respiratory reserve and demand and reflects neuromuscular drive for breathing and it is unaffected by respiratory compliance or resistance. Capdevila and colleagues [16] reported that patients with low P 0.1 and P 0.1 /MIP failed extubation, Mergoni and colleagues [30] reported excellent prediction of success in weaning using P 0.1 /MIP, while Del Rosario [31] found similar P 0.1 /MIP values in patients with weaning success and failure. In a metaanalysis, [26] P 0.1 /MIP ratio of >0.3 had a pooled likelihood ratio of 2.3, indicating increased chances of successful extubation. Despite excellent predictive accuracy, the role of P 0.1 /MIP ratio may be limited in most ICUs due to need for a special device.
Minute ventilation recovery time (V E RT)
Minute ventilation recovery time (V E RT) allows physiologic assessment of work imposed after SBT. Thus V E RT may identify patients with better respiratory muscle reserve, capable of sustaining spontaneous breathing following extubation. Martinez and colleagues, [2] after a 2-h SBT, placed patients back on their pre-SBT ventilator settings for up to 25 min and measured various respiratory parameters including minute ventilation (V E ) at three intervals: baseline over preceding 24 h (pre-SBT), post-trial (after SBT) and recovery (return to baseline). Patients were assumed to recover when V E decreased to 110% of the predetermined baseline. V E RT of patients with successful extubation was significantly shorter than those who failed extubation (3.6 ± 2.7 min vs. 9.6 ± 5.8 min, P < 0.011). On multivariate analysis, V E RT was an independent predictor of extubation outcome and correlated with ICU LOS ( P < 0.01). Prolonged V E RT may reflect either a limited respiratory reserve or an unrecognized, underlying disease process. Seymour and colleagues [32] evaluated a more practical method. For pre-SBT V E they collected data in three ways, a 24-h nadir (as in previous study), an 8-h average and the last V E measurement prior to SBT. They also collected data on V E RT with threshold of 100% and 110%. They found that both, the 8-h average V E and immediate pre-SBT value of V E, were in close agreement with the original method. Similarly 100% threshold for V E RT also correlated well with 110% threshold. The same group later demonstrated [33] the utility of the new method in predicting extubation success. Recently Hernandez and colleagues [34] evaluated the utility of close observation of V E during the recovery phase after the SBT. Both V E RT RT50% ∆V E (recovery time needed to reduce V E to half the difference between End-SBT- V E and basal V E ) were significantly lower in successfully extubated patients. They found that a threshold of RT50% ∆V E of seven minutes was useful to discriminate between extubation failures and successes. V E RT and derivatives appear to be promising tools, the drawback being their inability to identify patients with possible upper airway compromise.
Work of breathing (WOB)
Kirton and others [35] found that patients who fail SBT due to increased imposed work of breathing (WOB) secondary to ventilatory apparatus and endotracheal tube, but have normal physiological WOB, can be successfully extubated. The same group later showed [36] that when physiological WOB ≤0.8 J/l, patients can be successfully extubated. Automatic Tube Compensation (ATC), a form of variable pressure support, was shown [37] to improve extubation success by reducing imposed work of breathing. WOB, a promising predictor; remains confined to the research setting due to technical difficulties.
Displacement of liver/spleen
Diaphragm fatigue results in slower movement and reduced excursion. Jiang and colleagues [38] hypothesized that liver and spleen displacement during SBT can be a surrogate of diaphragmatic endurance. In 55 ICU patients, two separate observers measured the displacement of liver and spleen by ultrasonography. Patients were extubated by clinicians blinded to the study results. Patients who were successfully extubated had higher mean values. With a cutoff value of 1.1 cm, the sensitivity and specificity to predict successful extubation was 84.4% and 82.6%. This is a noninvasive test and can be done bedside, but needs expertise.extu
Extubation criteria
1) patient spontaneously ventilating
2) reversed adequately: sustained tetany w/o fade > 5 sec is one way to do it.
3) vital signs stable
4) not in stage 2
Book stuff:
RSBI < 100. Respiration rate/tidal volume in Liters.
nif <-20mmhg (you can take off bag and cover hole with hand and have patient suck in while watching pressure gauge
leak test for airway surgeries/long prone case (dunno how useful it is in reality)
Patient either deep or awake
Patient either breathing or easy to ventilate manually
Oral airway in place
Pharynx suctioned
Cuff deflated
Lungs manually inflated with 100% O2
Succinylcholine available.
NEVER extubate a patient without an oral airway in place. AFTER you extubate a patient, suction the pharynx one more time, put the mask on the patient, keep your right hand on the bag, test for airway patency, and then help them breathe for a while.
2) reversed adequately: sustained tetany w/o fade > 5 sec is one way to do it.
3) vital signs stable
4) not in stage 2
Book stuff:
RSBI < 100. Respiration rate/tidal volume in Liters.
nif <-20mmhg (you can take off bag and cover hole with hand and have patient suck in while watching pressure gauge
leak test for airway surgeries/long prone case (dunno how useful it is in reality)
Extubation Criteria
| Head lift, Grip |
| NIF < -25 torr |
| RR < 30 |
| TV > 5 cc/kg |
| VC > 10 cc/kg |
| PaO2 > 65 on FiO2 < .40 |
| PaCO2 < 50 torr |
| Resting MV < 10 l/min |
| Level of Consciousness OK |
| Muscle Relaxants OK |
| TV/RR > 10 |
Patient either deep or awake
Patient either breathing or easy to ventilate manually
Oral airway in place
Pharynx suctioned
Cuff deflated
Lungs manually inflated with 100% O2
Succinylcholine available.
NEVER extubate a patient without an oral airway in place. AFTER you extubate a patient, suction the pharynx one more time, put the mask on the patient, keep your right hand on the bag, test for airway patency, and then help them breathe for a while.
Saturday, October 15, 2011
Penicillin Allergy
Administration of a cephalosporin to a patient with a history of penicillin allergy
Sunday, October 9, 2011
A-a gradient
A-a O2 Gradient = [ (FiO2) * (Atmospheric Pressure - H2O Pressure) - (PaCO2/0.8) ] - PaO2 from ABG
Aa Gradient = (150 - 5/4(PCO2)) - PaO2
Normal Gradient Estimate = (Age/4) + 4
The 5 Causes of Hypoxemia, #1-3 have an elevated A-a Gradient:
V/Q Mismatch (ex: PNA, CHF, ARDS, atelectasis, etc)
Shunt (ex: PFO, ASD, PE, pulmonary AVMs)
Alveolar Hypoventilation (ex: interstitial lung dz, environmental lung dz, PCP PNA)
Hypoventilation (ex: COPD, CNS d/o, neuromuscular dz, etc)
Low FiO2 (ex: high altitude)
CO calculation usng Fick principle
http://www.josephsunny.com/medsoft/cardiology.html
Cardiac Output (Fick) in L/min = (135 ml O2/min/M2*BSA)/(13*Hgb*(SaO2-SvO2))
Cardiac Output (Fick) in L/min = (135 ml O2/min/M2*BSA)/(13*Hgb*(SaO2-SvO2))

- A commonly-used value for O2 consumption at rest is 125 or 135 ml O2 per minute per square meter of body surface area.
- The calculation of the arterial and venous oxygen concentration of the blood is a straightforward process. Almost all oxygen in the blood is bound to hemoglobin molecules in the red blood cells. Measuring the content of hemoglobin in the blood and the percentage of saturation of hemoglobin (the oxygen saturation of the blood) is a simple process and is readily available to physicians. Using the fact that each gram of hemoglobin can carry 1.36 ml of O2, the oxygen content of the blood (either arterial or venous) can be estimated by the following formula:
Assuming a hemoglobin concentration of 15g/dl and an oxygen saturation of 99%, the oxygen concentration of arterial blood is approximately 200ml of O2 per litre.
The saturation of mixed venous blood is approximately 75% in health. Using this value in the above equation, the oxygen concentration of mixed venous blood is approximately 150ml of O2 per litre.
Friday, September 30, 2011


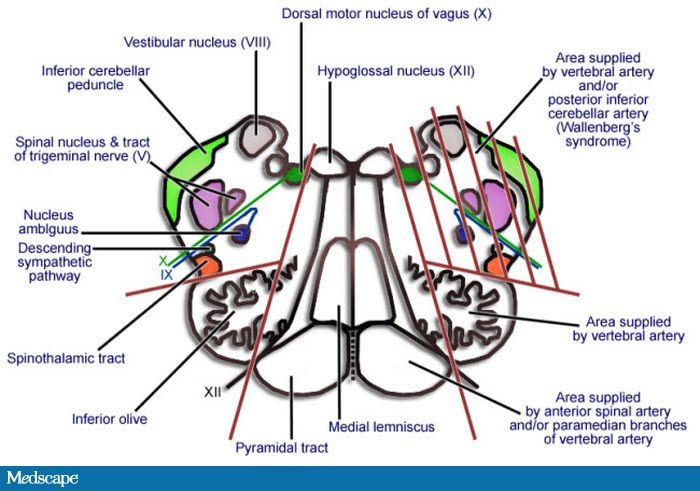
SYNDROMES
Wyburn–Mason syndrome: This congenital, nonhereditary disorder stems from a developmental abnormality of the vascular mesoderm in the optic cup and neural tube. This constellation of ipsilateral–intraorbital and cerebral arteriovenous malformations, which is often associated with facial nevi,
Wednesday, September 28, 2011
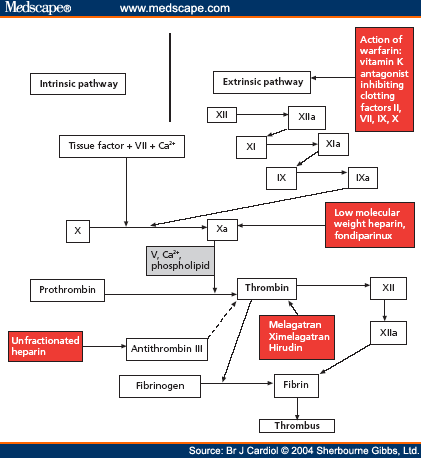
Pradaxa
Dabigatran (Pradaxa in Australia, Europe and USA, Pradax in Canada, Prazaxa in Japan) is an anticoagulant from the class of the direct thrombin inhibitors. It is being studied for various clinical indications and in some cases it offers an alternative to warfarin as the preferred orally administered anticoagulant ("blood thinner") since it does not require frequent blood tests for international normalized ratio (INR) monitoring while offering similar results in terms of efficacy
fondaparinaux
One potential advantage of fondaparinux over LMWH or unfractionated heparin is that the risk for heparin-induced thrombocytopenia (HIT) is substantially lower. Furthermore, there have been case reports of fondaparinux being used to anticoagulate patients with established HIT as it has no affinity to PF-4. However, its renal excretion precludes its use in patients with renal dysfunction.
Unlike direct factor Xa inhibitors, it mediates its effects indirectly through antithrombin III, but unlike heparin, it is selective for factor Xa.[1]
Heparin
An IV heparin protocol
When intravenous UFH is initiated for DVT anticoagulation, the goal is to achieve and maintain an elevated activated partial thromboplastin time (aPTT) of at least 1.5 times control. Heparin pharmacokinetics are complex, and the half-life is 60-90 minutes. A protocol for IV heparin use is as follows:
- Give an initial bolus of 80 U/kg.
- Initiate a constant maintenance infusion of 18 U/kg.
- Check the aPTT or heparin activity level 6 hours after the bolus, and adjust the infusion rate accordingly.
- Continue to check the aPTT or heparin activity level every 6 hours, until 2 successive values are therapeutic.
- Monitor the aPTT or heparin activity level, hematocrit, and platelet count every 24 hours.
Tuesday, September 27, 2011
Sunday, September 25, 2011
Thursday, September 22, 2011
FiO2 CALCULATIONS
For every 1 L/min of oxygen by NC, you add 3% to the estimated FiO2. So someone on 4L NC is getting about 33% FiO2 (21 + 12). Of course the FiO2 when you are talking about nasal canula is always an estimate, as people are variable in how much they breathe through their mouth. The actual FiO2 can vary quite a bit.
Wednesday, September 21, 2011
Sunday, September 11, 2011
INfective Endocarditis: Acute
So today I got one pt with IE..so lets discuss lil bit abt IE management:
Treatment:
Empiric treatment:
specific Treatment:
Usually Native valve endocariditis is caused by Strep Viridans and Bovis : can use
-Pen G alone If no other complication but require Continous IV infusion 12-18u/day or 6times a day for 4 weeks so has very poor pt compliance
- or ampicillin 12 gm/day as continous IV infusion or 6 equally divided doses iv
- can Use ceftriaxone in place of Pen G, and it requires only twice a day dose for sick and Once a day dose for Stable pt so has good pt compliance..sometimes can be given IM if IV access is difficult.
-cefazolin 6gm/day can be also used in 3 equally divided doses for 4 weeks
-if allergic to penicillin ; use vanco 30 mg/kg/day , but not more then 2gm/day q12hrly for 4 weeks
-for sick/complicated pt ahve to use 2 drugs so have to add genta 1 mg/kg with Pen G or Ceftriaxone
For enterococcal Infection:
same treatment can be used
if PVE: then 6 weeks of treatment is used
-A combination of an inhibitor of cell wall synthesis (ie, penicillin, vancomycin) with an aminoglycoside (ie, gentamicin, streptomycin) is necessary to achieve bactericidal activity against the enterococci. Tobramycin or amikacin does not act synergistically with antibiotics active against the bacterial cell wall.
-if resistnace to Beta lactmase then : use Ampi-sulbactam/vanco/cipro/imipenam + genta
For VRE:
Treatment:
Empiric treatment:
- for native valve endocarditis: Pen G+ genta--for synergistic coverage for strep
- for prosthetic valve: have to cover MRSA and Coag negative Staph aureus : so have to use Vanco+genta
- For IVDA: have to cover staph aureus: Nafcillin/vanco+ Genta
- rifampin can be added if pt has any foreign body: like prosthetic valve..as Rifampin can penetrate biofilm of most of the pathogen ...shoud be added to Vanco+gentaan
- can use Linezolid in place of vanco if renal function is not good and have difficulty in achieving trough level.
- if vanco resistance: then can use linezolid or Daptomycin
- have to give ABX for almost 4-6 weeks and Only IV treatment not oral ..Oral should be used only as suppressive for inoprable Prosthetic valve Endocarditis.
If pt has vagetation then it is difficult to eradicate oragnism as antibiotic had dofficulty in penetrating fibrin/platelet rich thrombi
specific Treatment:
Usually Native valve endocariditis is caused by Strep Viridans and Bovis : can use
-Pen G alone If no other complication but require Continous IV infusion 12-18u/day or 6times a day for 4 weeks so has very poor pt compliance
- or ampicillin 12 gm/day as continous IV infusion or 6 equally divided doses iv
- can Use ceftriaxone in place of Pen G, and it requires only twice a day dose for sick and Once a day dose for Stable pt so has good pt compliance..sometimes can be given IM if IV access is difficult.
-cefazolin 6gm/day can be also used in 3 equally divided doses for 4 weeks
-if allergic to penicillin ; use vanco 30 mg/kg/day , but not more then 2gm/day q12hrly for 4 weeks
-for sick/complicated pt ahve to use 2 drugs so have to add genta 1 mg/kg with Pen G or Ceftriaxone
For enterococcal Infection:
same treatment can be used
if PVE: then 6 weeks of treatment is used
-A combination of an inhibitor of cell wall synthesis (ie, penicillin, vancomycin) with an aminoglycoside (ie, gentamicin, streptomycin) is necessary to achieve bactericidal activity against the enterococci. Tobramycin or amikacin does not act synergistically with antibiotics active against the bacterial cell wall.
-if resistnace to Beta lactmase then : use Ampi-sulbactam/vanco/cipro/imipenam + genta
For VRE:
- can use Quinupristin/dalfopristin
- ampi+ceftriaxone
- ampi+ imipenam
- linezolid
- chloramphenical
For MSSA:
- Nafcillin/oxacillin 2gm/day q4hrly
- cefazolin 2gm IV q 8hrly
- if allergic to pen: use Vanco 30 mg.kg /day
Id staph with MIC for vanco> 1.5-2 mcg/ml ---use other ABX---linezolid/daptomycin
If PVE +MSSA:
use Cefazolin/nafcillin/oxacillin for 4-6 week
add Genta+ rifampicin for 2 week
PVE+MRSA:
use Vanco+ genta+rifampin
Linezolid had better outcome then Vanco: but have to monitor blood count
or daptomycin
HACEK:
use ampicillin or cefazolin
VAlve replacement Surgery:
if IE cause
- CHF
- >1cm vegetation
- perivalvular or myocardial abscess
- valve dysfunction
- >1 embolic episode
Fungal IE:
Surgical excision+ Amphotericin B
Daptomycin
Recently we discussed New drug Daptomycin...so I m Gonna post few facts regarding it:
MOA: cause Cell wall depolarization--> inhibit DNA, RNA and Protein synthrsis
Organism suscetibility: only gm +ve cocci--> staph-->MRSA too, Strep, ENterococci --also GRE
Used for MRSA, Rt sided endocarditis, soft tissue Infection...
Side effect:
Renal Failure
rhabdomyolysis---> so be careful while using dapto and statin together.
Limitation:
Cant be used in Pneumonia as It binds to surfactant ..
MOA: cause Cell wall depolarization--> inhibit DNA, RNA and Protein synthrsis
Organism suscetibility: only gm +ve cocci--> staph-->MRSA too, Strep, ENterococci --also GRE
Used for MRSA, Rt sided endocarditis, soft tissue Infection...
Side effect:
Renal Failure
rhabdomyolysis---> so be careful while using dapto and statin together.
Limitation:
Cant be used in Pneumonia as It binds to surfactant ..
Friday, September 9, 2011
Pulmonary HTN
Based upon a Doppler echocardiographic study, it can be determined if PH is likely, unlikely, or possible [8]:
- PH is likely if the PASP is >50 and the TRV is >3.4
- PH is unlikely if the PASP is ≤36, the TRV is ≤2.8, and there are no other suggestive findings
- PH is possible with other combinations of findings
- Pulmonary hypertension (PH) defined as a mean pulmonary arterial (PA) pressure of greater than 25 mm Hg at rest or greater than 30 mm Hg during exercise, is characterized by a progressive and sustained increase in pulmonary vascular resistance that eventually leads to right ventricular (RV) failure.
- Diagnosis of PAH requires the presence of pulmonary hypertension with two other conditions. Pulmonary artery occlusion pressure (PAOP or PCWP) must be less than 15 mm Hg (2000 Pa) and pulmonary vascular resistance (PVR) must be greater than 3 Wood units (240 dyn•s•cm−5 or 2.4 mN•s•cm−5).
Thyroid Nodule
Today I got case of Thyroid Nodule...She has < 1 cm nodule 1 year back and now it's 1.6 cm. , was solid, Normal TSH and T4. so biopsy was recommended..I m just posting algorithm for management of tHyroid nodule

Wednesday, August 31, 2011

pseudomonas infection
Antimicrobial agents are needed to treat Pseudomonas infections. Two antipseudomonal drug combination therapy (eg, a beta-lactam antibiotic with an aminoglycoside) is usually recommended for the initial empiric treatment of a pseudomonal infection, especially for patients with neutropenia, bacteremia, sepsis, severe upper respiratory infections (URIs), or abscess formation. The choice of antibiotic also depends on the site and extent of infection and on local resistance patterns.[5] Reports of more resistant strains of Pseudomonas organisms to the currently used antimicrobials are causing much concern.
B cepacia has grown resistant to aminoglycosides, antipseudomonal penicillins, and most beta-lactam agents. Some strains are variably susceptible to third-generation cephalosporins, ciprofloxacin, trimethoprim-sulfamethoxazole, ampicillin-sulbactam, chloramphenicol, or meropenem.
Because human cases of glanders are rare, limited information is available about antibiotic treatment of the organism in humans. Sulfadiazine has been effective in experimental treatments of animals and humans. B malleiorganisms are usually sensitive to tetracyclines, ciprofloxacin, streptomycin, novobiocin, gentamicin, imipenem, ceftazidime, and sulfonamides. Resistance to chloramphenicol has been reported. Treatment duration is often prolonged, from 1-2 months, often combined with surgical drainage.
Ceftazidime alone or in combination with either trimethoprim-sulfamethoxazole or amoxicillin clavulanate is the therapy of choice for B pseudomallei. The organism is usually sensitive to imipenem, penicillin, doxycycline, azlocillin, ceftazidime, ticarcillin-clavulanic acid, and ceftriaxone. Initiate treatment early in the course of the disease. The organism is resistant to ciprofloxacin and aztreonam. Treatment is often prolonged, from 3-12 months, with the longest duration of therapy used for chronic extrapulmonary disease.
Pseudomonas vaccines are also currently used to reduce infection risks in patients with cystic fibrosis (CF) and are still under investigation.Pseudomonas aeruginosa infections include the following:
- Bacteremia
- Empiric antibiotics are often started before the organism is identified.
- Whether single-drug or combination therapy is most effective in patients who have bacteremia and neutropenia is debated. The author is unaware of any prospective randomized comparison between monotherapy and combination drug therapy for patients with pseudomonal bacteremia. Duration of treatment is at least 2 weeks.
- Bone and skin infections
- A 4-week course of aminoglycoside antibiotics is often successful for managing vertebral osteomyelitis.
- Sternoarticular pyarthrosis has been managed effectively with aminoglycoside and antipseudomonal penicillin if administered for at least 6 weeks.
- Patients with osteomyelitis of the pubic symphysis require treatment for at least 4 weeks with an antipseudomonal penicillin and aminoglycoside combination. Surgical intervention is not usually indicated.
- Patients with osteochondritis require medical and surgical treatment. Parenteral administration of 1-2 antipseudomonal agents is recommended before surgical debridement. The recommended regimen continues postsurgical treatment for 1-2 additional weeks with oral (PO) ciprofloxacin.
- Chronic contiguous pseudomonal osteomyelitis requires 4-6 weeks of combination therapy, in addition to surgical debridement.
- Burn wound sepsis management requires early intervention with daily wound inspection and systemic antibiotic combination regimens. Monotherapy is not indicated.
- Management of pseudomonal cellulitis includes the use of PO antibiotic for 7-10 days; this often resolves a localized infection.
- Pseudomonal toe web infections require initial debridement with applications of silver nitrate or 5% acetic acid to the toe webs and the dorsal and planter areas. Following this initial treatment, apply a topical antibiotic, silver sulfadiazine cream, or Castellani paint until infection resolves. PO quinolone effectively reduces the duration of infection.
- Pseudomonal folliculitis is often self-limited; treatment may require only application of silver sulfadiazine cream or 5% acetic acid wet compresses for 20 minutes 2-4 times daily with topical antibiotics.
- CNS infections
- Ceftazidime, cefepime, or meropenem are the antibiotics of choice because of their high CNS penetration. Initially, consider double coverage with an aminoglycoside for patients with adequate renal function. Aztreonam, ciprofloxacin, or levofloxacin are indicated for patients with renal failure and those allergic to beta-lactam. Imipenem-cilastatin should be avoided because of the risk of seizures. Intrathecal treatment should also be considered. Treatment duration should be at least 2 weeks.
- Antibiotics can be used in the initial treatment of brain abscesses that are multiple, small (ie, < 2 cm), poorly distributed, or relatively difficult to access. Antibiotic therapy duration depends on the speed of abscess shrinkage, but therapy usually lasts 2-6 weeks.
- Ear and eye infections
- Otitis media in at-risk populations should be treated with antipseudomonal agents for at least 10 days.
- Chronic suppurative otitis media requires daily aural toilet and treatment with antibiotics (eg, ceftazidime, mezlocillin, ciprofloxacin), and often surgical treatment.
- Otitis externa can be treated with local care using an acetic acid compress and daily aural cleaning.
- Management of malignant externa otitis should be aggressive and involve both medical and surgical therapies. The conventional therapy (ie, an aminoglycoside and a beta-lactam agent with antipseudomonal activity) is needed for at least 4 weeks to treat localized infections and 6-8 weeks or longer to treat extensive disease. Monotherapy using ceftazidime intravenously (IV), cefepime IV, or ciprofloxacin PO for 6 weeks has been reported effective.
- If gram-negative rods are isolated from the Gram stain of an eye infection, immediately start a combined topical and subconjunctival (or subtenon) therapy of aminoglycoside antibiotics. Aminoglycoside solution (not ointment) must be applied to the affected eye every 30-60 minutes. Subconjunctival therapy is needed for the first 3 days of treatment. Total duration of therapy is at least 1 week. An alternative therapy uses a quinolone antibiotic solution. The addition of parental or PO antipseudomonal antibiotics also has been beneficial.
- Pseudomonal endophthalmitis requires immediate antibiotic therapy, using aminoglycoside and antipseudomonal penicillin administered via a parenteral and subconjunctival, topical, or intraocular route. Therapy duration depends on the clinical improvement.
- GI and GU infections
- Treat GI manifestations of pseudomonal infection with antibiotic therapy for patients with severe localized or systemic infections.
- The treatment modality for urinary tract infection (UTI) depends on the presence of sepsis, degree of chronicity, potential sites of persistent infection, and local antibiotic susceptibility. Ideally, indwelling urinary catheters should be removed. If the catheter cannot be removed, consider treating only symptomatic episodes or exacerbations because it is not feasible to totally eradicate the organism. Aminoglycosides and quinolones remain the agents of choice.
- Cardiovascular (CV) and respiratory infections
- To treat endocarditis, administer an antipseudomonal beta-lactam with high-dose aminoglycoside for approximately 6 weeks.
- According to the criteria used in France to select antibiotics to treat VAP, the following 2 risk factors must be considered: (1) administration of broad-spectrum antibiotics in the previous 15 days and (2) mechanical ventilation for fewer than 7 days or for 7 or more days. The extended factors predict the involvement of multiresistant nosocomial P aeruginosa, suggesting administration of carbapenems to those who have undergone mechanical ventilation of 7 or more days and who have been exposed to antibiotics in the prior 15 days.
- The role of antibiotic prophylaxis or chronic suppression of respiratory pseudomonal infections in patients with CF is controversial. Among the promising treatment plans are intermittent aerosolization of antibiotics to patients with CF who have established pseudomonal lung infections.
- Choices for empiric antibiotic treatment in patients with a history of Pseudomonas infection requires review of previous culture sensitivity.
- More widely accepted is the treatment of children with pseudomonal infections by using fluoroquinolone, especially children with previous therapeutic failure or resistance to multiple other antibiotics.[6] Treatment often continues until symptoms resolve (ie, 1-2 wk).
- Inhalation of mucolytic and hydrating agents, postural drainage, and chest physiotherapy often are therapies used together. Bronchial lavage also has been used to remove respiratory secretions.