Recently I came across this interesting case where patient had Hemorrhagic stroke and also had repolarization defects -- QT prolongation, T wave inversion..---in her ECG....Quite interesting huh!!!
so here is the case ( from Medscape):
so here is the case ( from Medscape):
An 81-year-old woman presents to the emergency department (ED) with an altered mental status. The patient was in her usual state of health until she vomited several times earlier today. Her family attributed the vomiting to discontinuation of her metoclopramide therapy, which she was taking for diabetic gastroparesis. The medication was stopped because the patient's family was concerned that this medication was aggravating her facial dyskinesia. As the day progressed, the patient was noted to have difficulty communicating; she could neither understand commands nor verbalize simple phrases. In addition, she was noted to be unable to move her left upper extremity. The patient lives alone. She has no documented history of trauma but does have a history of repeated falls. She has a medical history of end-stage renal disease requiring hemodialysis, insulin-dependent diabetes mellitus, hypertension, and coronary artery disease that is poorly defined. Her medications include aspirin, insulin, sevelamer hydrochloride, simvastatin, labetalol, and enalapril.
On physical examination, the patient appears ill, with a temperature of 98.4°F (36.9°C), a blood pressure of 180/89 mm Hg, a heart rate of 72 bpm, and a respiratory rate of 14 breaths/min. Her oxygen saturation is 96% while breathing room air. The findings of the pulmonary, cardiac, and abdominal examinations are within normal limits. The neurologic examination, however, reveals a patient that is aphasic and has left hemiparesis. Her finger-stick blood glucose level is 112 mg/dL (6.2 mmol/L).
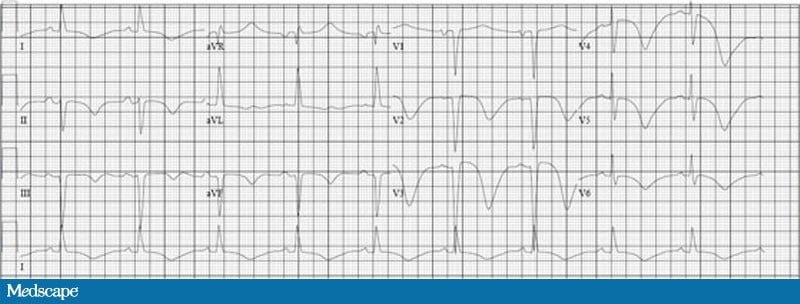
An electrocardiogram (ECG) is ordered:
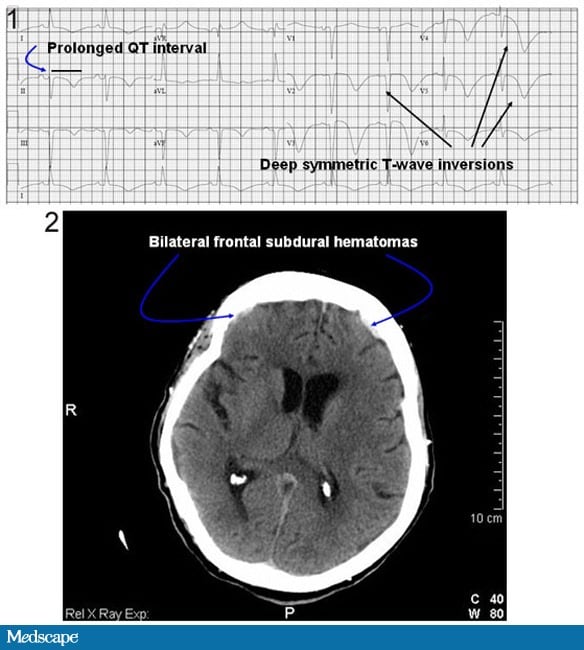
The patient's ECG demonstrated a sinus rhythm at a rate of 60 bpm, with a markedly prolonged QT interval of 680 msec (normal range for females, <470 msec) and deep, symmetric T-wave inversions most pronounced in the anterior precordial leads (V2-V6). Because of the patient's altered mental status and focal neurologic findings, a noncontrast computed tomography (CT) scan of the head was obtained, which demonstrated bilateral, frontal subdural hemorrhages
The patient in this case was admitted to the intensive care unit for cardiac monitoring, serial neurologic examinations, and further testing. An MRI of the brain confirmed a right-sided acute ischemic stroke, but the presence of the small subdural hemorrhages (likely the result of the patient's recurrent falls) prevented the use of antiplatelet therapy in this patient. The ECG changes normalized within 2 days and the cardiac enzymes remained within normal limits. An echocardiogram was performed on hospital day 2 which demonstrated moderate diastolic dysfunction, with no focal wall motion abnormalities. A repeat CT scan of the head on hospital day 4 showed no progression of the small subdural hemorrhages. The patient's neurologic exam did not change from her initial presentation and she was discharged to a skilled nursing facility on hospital day 5.
The pathogenesis of ECG changes and cardiac arrhythmia in the setting of a CNS event involves alterations in the complex neural-cardiac pathways that are responsible for normal autonomic control of cardiac function. In the setting of acute stroke, autonomic tone is dysregulated by a predominant adrenergic surge of catecholamines (such as norepinephrine). In particular, involvement of the insular cortex by the CNS event is commonly associated with a surge in norepinephrine, and it is associated with an increased rate of arrhythmias and death.
Adrenergic overstimulation may lead to ventricular systolic dysfunction and wall motion abnormalities, with or without serum biochemical markers of myocardial necrosis. The classic description of adrenergically mediated cardiac dysfunction is termed "takotsubo cardiomyopathy"; it presents with apical wall motion abnormalities in the setting of severe emotional stress.
A recent report described a presentation of takotsubo-like apical ballooning in association with ischemic-like ECG changes and elevated serum cardiac biomarkers in the setting of acute subarachnoid hemorrhage.
Despite marked cardiac wall motion abnormalities during the acute presentation, a repeat echocardiogram 1 week after the event showed complete resolution of the cardiac regional wall motion abnormalities. The presence of regional wall motion abnormalities during acute stroke is a well-described entity. Kono et al performed coronary angiography in 12 patients with acute stroke symptoms and the presence of ischemic ECG changes and regional wall motion abnormalities. Despite the presence of focal wall motion abnormalities, none of these patients demonstrated significant coronary artery stenosis or evidence of coronary vasospasm. On follow-up echocardiographic examination, the regional wall motion abnormalities in these patients had resolved.
Treatments aimed at limiting adrenergic stimulation to the heart (beta-adrenergic receptor antagonists) can be given if the patient manifests evidence of cardiac dysfunction or injury. In cases of severe systolic dysfunction, supportive measures such as loop diuretics, supplemental oxygen, and/or endotracheal intubation may be necessary. While no randomized data support their use in stroke-mediated cardiac dysfunction, angiotensin-converting enzyme inhibitors (ACEI) and statin therapy are also reasonable options.[
No comments:
Post a Comment